Results of a prospective study of de Quervain’s Tenosynovitis completed at Bondi Junction Hand Therapy
Hand therapy plays an important role in the recovery form de Quervain’s. At Bondi Junction Hand Therapy (BJHT) we see a lot of patients with de Quervain’s and at the start of 2014 we began a prospective study to collect data on our de Quervain’s patients and their recovery. Below is a summary of hand therapy intervention for de Quervain’s followed by information about the research.
Hand Therapy and de Quervain’s
- Hand therapy is an important component of treating de Quervain’s. Time is spent with each patient to assess their level of impairment (reduced strength, tightness of affected muscle tendon units), and importantly daily activities that may be contributing to their condition (baby handling, work set-up).
- Hand therapists do not discourage patients from seeking other treatment, and can be an important source of education and information. Hand therapy is multi-faceted in the approach to de Quervain’s; and all treatment options are discussed with patients to increase their knowledge and understanding of their condition and what is available to them.
- Not all patients require a Cortisone Injection or surgery to recover from de Quervain’s. Some patients respond very well to conservative treatment and recover through a variety of therapeutic approaches.
- Hand therapy can complement other treatments (Cortico Steroid Injection (CSI), Surgery). After a CSI some patients require splinting or strengthening to fully recover. Some patients have weakness &/or sensitive scars post-surgery and benefit from strengthening and desensitisation.
Hand Therapy for de Quervain’s
- Patient education (including baby handling, activity/ work modification techniques)
- Customised splinting
- Stretches & Strengthening exercises
- Dynamic taping
Prospective Study
Below is a brief outline of the study and the initial results; the study will be published in more detail at a later stage.
Background
At Bondi Junction Hand Therapy (BJHT) a significant number of parents with babies less than twelve months old present with de Quervain’s (deQ). It was our perception that 35-40 year old mothers with babies under twelve months were the majority of the deQ population seen at BJHT. This population are not always interested in injections or surgery and we were interested in the following questions:
- Current literature on the treatment of de Quervain’s
- How many patients recover without injections or surgery
- What is the demographics of patients presenting with de Quervain’s to the practice, and does this reflect the literature
- Is there an outcome measure that is quick and simple to measure changes in patients recovery
Literature
- Literature searches on de Quervain’s treatment outlines cortisone steroid injections (CSI) mostly and surgery if CSIs fail; however many patients do not have either and recover with conservative treatment.
Where is the research on the effectiveness of splinting and hand therapy alone and/or to support patients who need therapy in addition to a CSI or surgery?
Method
Data was collected at the initial appointment, then at six weeks, six and twelve months. All patients who presented with only de Quervain’s with no prior deQ surgery. Between January 2014 and March 2015 these patients had their initial data recorded, and follow-ups were collected until the end of April 2015.
48 sets of initial data were collected and 44 sets of follow-up ranging from six weeks to twelve months post initial appointment.
The information collected included:
- Age
- Gender
- Parent of a <12month baby
- Grip strength to onset of pain
- Dominant/ non-dominant/ bilateral side affected
- QuickDASH outcome measure score
- Time since symptoms started
- Corticosteroid Injection history
- Splint wearing status
All initial data was collected face to face. The study was explained, consent gained and a study information sheet provided.
Data was collected face to face if patients were still attending therapy, however 50% of the follow-up data was obtained using an online survey through SurveyMonkey.
It is impossible to know why patients did or did not complete the survey and if this was a reflection on their recovery.
As a small and busy private practice it was difficult to find the time for clinicians to contact patients for follow-up data, and after 15months, it was decided to focus on the initial data obtained and wind-up the collection.
This obviously skews the follow-up results, however as clinicians we found the initial data valuable.
The demographics
De Quervain’s is most common between the ages of 30 to 50 years and females are ten times more likely to have the condition. The age range during our study had a wide age range of 17 to 77 years but the mean of 36.5 years did fall within the range age from the literature, and the gender ratio was also consistent.
63% of the e Quervain’s patients who attended hand therapy with only deQ were parents with babies 12 months or under, making up a significant percentage for this condition. There were mothers and fathers who were affected, and all patients who had de Quervain’s bilaterally were parents.
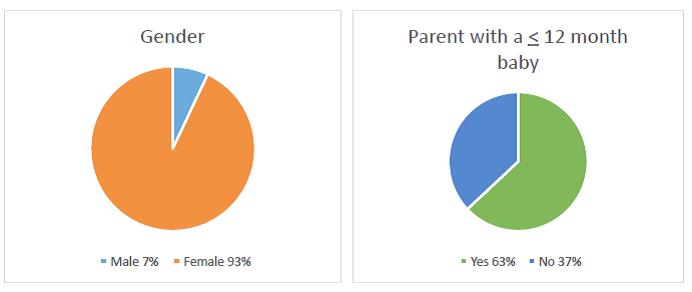
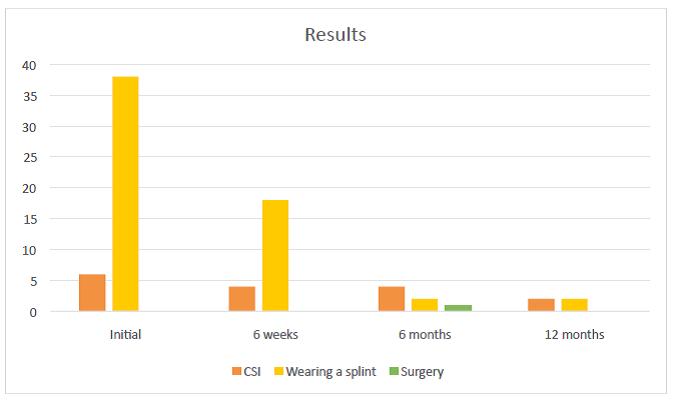
Initial Results
63% of the patients presenting with deQ were parents with a baby 12months or younger. While most of the parents were mothers, fathers were not immune.
Prior to hand therapy treatment six (12.5%) of the patients had received a steroid injection.
39 (81%) went into a splint at the initial appointment, and this included all of the six patients who had already has a Cortico Steroid Injection.
The QuickDASH Outcome Measure: in the general population a score of 10.1 is considered normal. The mean at the initial appointment was 40.31, indicating it is sensitive to the effects of de Quervain’s and therefore shows the impact of de Quervain’s on upper limb function. Throughout the follow-up a consistent decrease in the mean QuickDASH score was observed.
Most patients only had one hand affected, 52% had their dominant hand affected, however 10% of the participants had bilateral injuries and these were all parents of babies twelve months or younger.
Patients presented to hand therapy between zero – weeks since the pain had started, with a mean of 8.5 weeks.
Summary
- Hand therapy can complement other treatments (CSI, Surgery)
- Hand therapy is an important component of treating de Quervain’s
- Hand therapists do not discourage patients from seeking other treatment, and can be an important source of education and information
- Not all patients require a CSI or surgery to recover from de Quervain’s
Reference List
Beaton D.E., Wright J.G., Katz J.N. Development of the QuickDASH: Comparison of Three Item-Reduction Approaches. Journal of Bone and Joint Surgery. May 2005; 87, 5; pp 1038-1046.
Huisstede B.M., van Middelkoop M, Randsdorp M.S., Glerum S., &Koes B.W. Effectiveness of Interventions of Specific Complaints of Arm, Neck&/or Shoulder: 3 Musculoskeletal Disorders of the Hand. Physical Medicine and Rehabilitation, Vol 91, 2010 pp298-314.
O’Brien L, Hardman A, &Goldby S. The impact of a hand therapy screening and management clinic for patients referred for surgical opinion in an Australian public hospital. Journal of Hand Therapy 26 (2013) 318e322
Richie C.A., & Briner W.W., Corticosteroid Injection for Treatment of de Quervain’s Tenosynovitis: A Pooled Quantitative Literature Evaluation. Journal of the American Board of Family Medicine, 16:102-106, 2003.
Pensak M.J., Bayron J., & Wolf J. M. Current Treatment of de Quervain Tendinopathy.
The DASH Outcome Measure. http://dash.iwh.on.ca/quickdash . Accessed December 2013.
Stahl S., Vida D., Meisner C., Lotter O., Rothenberger J., Schaller H. & Stahl A. S. Systematic Review and Meta-Analysis on the Work-Related Cause of de Quervain Tenosynovitis: A Critical Appraisal of Its Recognition as an Occupational Disease. Plastic and Reconstructive Surgery Journal, 2013.



