Scaphoid fractures are common, accounting for at least 75% carpal fractures (Rhemrev et al., 2011, Alshryda et al., 2012), and usually occur as a consequence of a fall onto an outstretched hand. So scaphoid fractures are frequently seen, can be difficult to diagnose, and may not heal despite management. Rhemrev et al., (2011) reports the non-union rate between 5 -15%. Because of this,and the associated early onset arthritis associated with scaphoid non-union, it’s important to know which type of scaphoid fractures do well with casting, and when to refer on. It’s also important to know the type of cast that should be used in managing the scaphoid fracture conservatively.
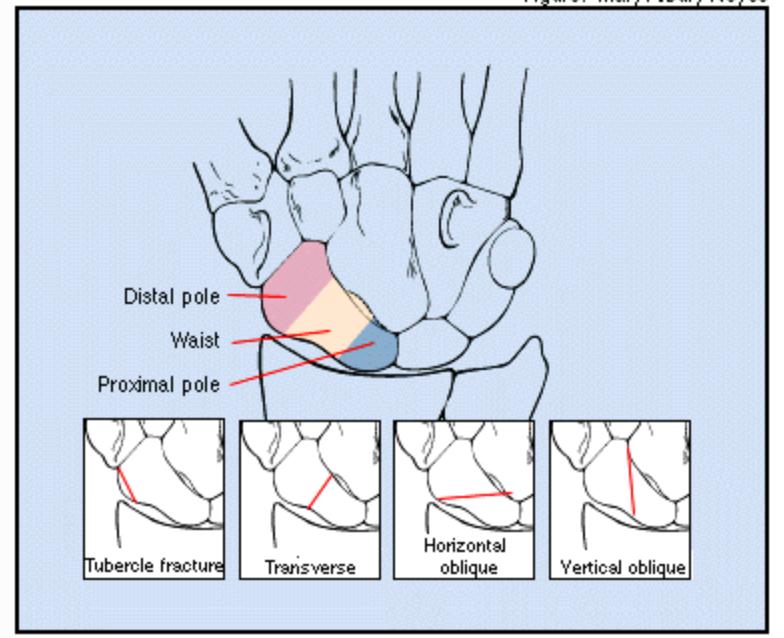
The acute non-displaced waist fracture, distal scaphoid fractures and scaphoid tuberosity fractures are typically managed with casting (Dell et al., 2011), while displaced fractures, those with delayed presentation for treatment and proximal pole fractures are less likely to do well with casting and should be reviewed by a hand surgeon for possible surgical intervention (Tan et al., 2009).
When casting is appropriate, the type of cast needs consideration. Alshryda et al., (2012) using a meta-analysis concluded no benefit of an above elbow cast over a below elbow cast for managing scaphoid fractures. A short arm cast that has the thumb free is better tolerated by patients as it allows more function compared to a thumb spica cast (Rhemrev et al., 2011). There has been a number of studies assessing the need to include the thumb as part of casting for the non-displaced scaphoid fracture. There have been biomechanical cadaveric studies as well as prospective prognostic studies that have tried to help answer this question.
Schramm et al., 2008 used CT scans to assess the effect of load on cadaveric transverse waist fractures and compared no immobilisation, short arm cast with thumb free and thumb spica casting. They found immobilising the wrist crucial to limit fracture fragment mobility, but no difference between the short arm cast compared with the thumb spica cast.
Clay et al., 1991 in a prospective randomised trial of 392 non-displaced scaphoid waist fractures found the union rate for both groups to be 90%. Ram & Chung, (2009) reviewed the RCT and quasi RCT studies of non-displaced scaphoid fractures, and would apply a short arm cast that leaves the thumb free to the level of the mcp joint. The position of the wrist would be in slight extension as it enables function and doesn’t hinder fracture healing (Hambidge et al, 1991). If fracture union is uncertain at 8 weeks, a CT scan should be considered, and if there is a gap seen on CT, surgery may be offered.
So in summary, acute non-displaced waist or distal scaphoid fractures can be treated with casting, and the literature suggests a short arm cast up excluding the thumb provides sufficient immobilisation of the healing scaphoid fracture.
References
Alshryda, S., Shah, A., Odak, S., Al-Shryda, J., Ilango, B. & Muralia, S.R. (2012). Acute fractures of the scaphoid bone: Systematic review and meta-analysis. The Surgeon, Journal of the Royal Colleges of Surgeons of Edinburgh and Ireland, 10:218-229.
Clay NR, Dias JJ, Costigan PS, Gregg PJ, Barton NJ. Need the thumb be immobilised in scaphoid fractures? Journal of Bone Joint Surgery Am 1991: 73B:828-32
Dell, P., Dell, R. & Griggs, R. (2011). Management of Carpal Fractures and Dislocations. In Skirven, Osterman, Fedorczyk & Amadio (Eds), Rehabilitation of the Hand and Upper Extremity (pp. 988-1001).
Hambidge JE, Desai VV, Schranz PF, Compson JP, Davis TR, Barton NJ. Acute fractures of the scaphoid. Treatment by cast immobilization with the wrist in flexion or extension? J Bone Joint Surg Br 1999;81:91–2.
Ram AN, Chung KC; Evidence-based Management of Acute Non-displaced Scaphoid Waist Fractures. Journal of Hand Surgery AM 2009, April 34(4); 735-738.
Schramm et al., (2008) Does thumb immobilisation contribute to scaphoid fracture stability Hand 2008 March 3(1) 41-43
Tan, S., Craigen, M.A.C., & Porter, K. (2009). Acute scaphoid fracture: a review. Trauma, 11: 221-239.



